Editor’s Note (12/21/21): This article is being showcased in a special collection about equity in health care that was made possible by the support of Takeda Pharmaceuticals. The article was published independently and without sponsorship.
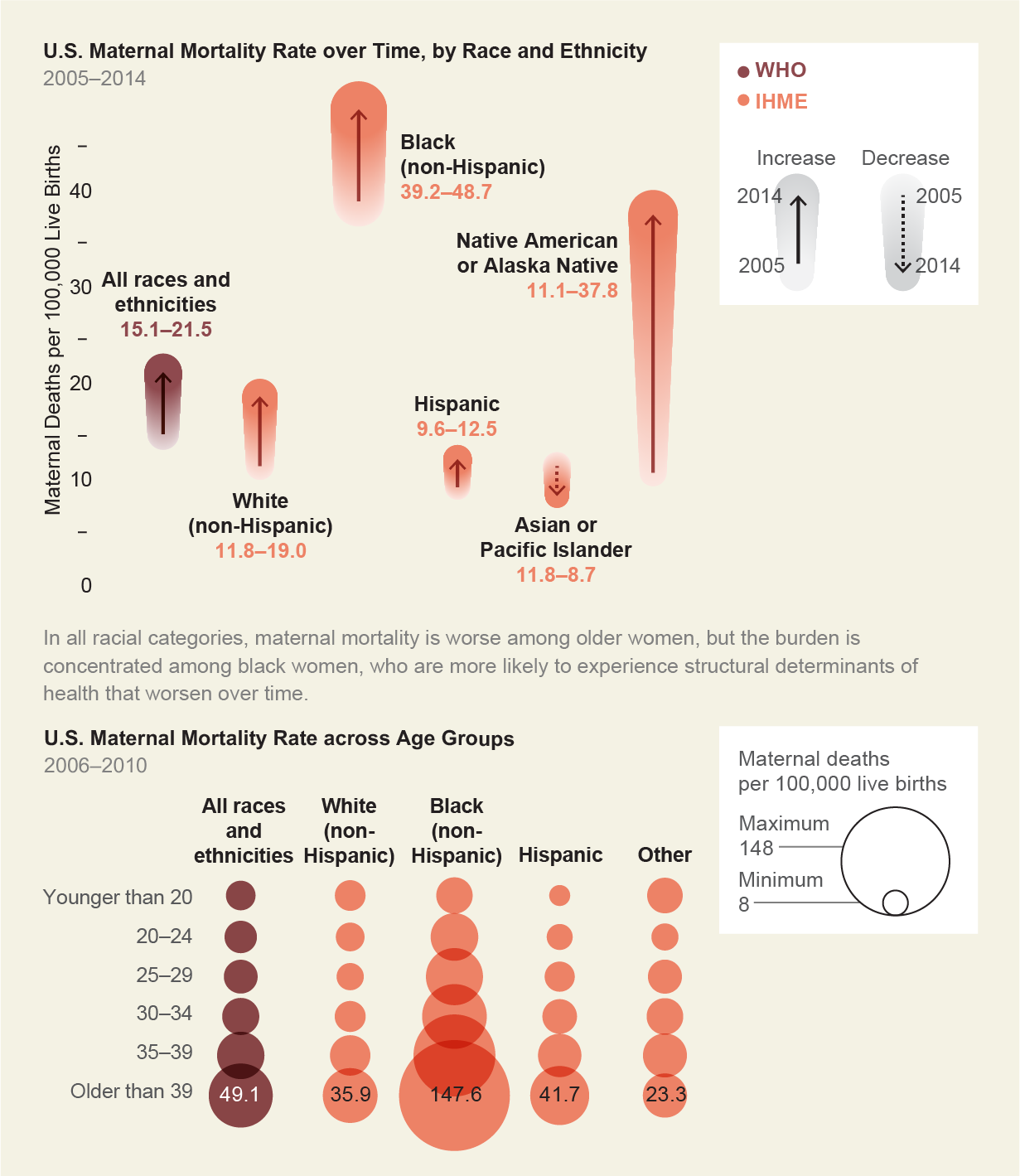
The shameful secret is out: Although the number of women who die in childbirth globally has fallen in recent decades, the rates in the U.S. have gone up. Since 1987 maternal mortality has doubled in the U.S. Now approximately 800 maternal deaths occur every year. One of the most striking takeaways from examining the data is racial disparity: Black women are three to four times more likely to die from pregnancy-related conditions such as cardiac issues and hemorrhage and to bear the brunt of serious complications. That risk is equally shared by all Black women regardless of income, education or geographical location. In other words, the factors that typically protect people during pregnancy are not protective for Black women.
Fortunately, most of these deaths are considered preventable, and therefore much more can be done to stop them. First, everyone—from doctors to the media to the public—needs to stop blaming women for their own deaths. Instead we should focus on better understanding the underlying contributing factors. These include a lack of data; not educating patients about signs and symptoms—and not believing them when they speak up; errors made by health-care providers; and poor communication among different health-care teams. Finally, studies have shown that interventions such as wider access to midwifery, group prenatal care, and social and doula support are effective in improving maternal health outcomes.
Progress has been slow and uneven. Deaths from hemorrhage, for example, have been reduced by half in some states because of standardized tool kits for care. And California has led in the pursuit of understanding root causes of maternal mortality. Still, structural racism is proving to be an intractable force.
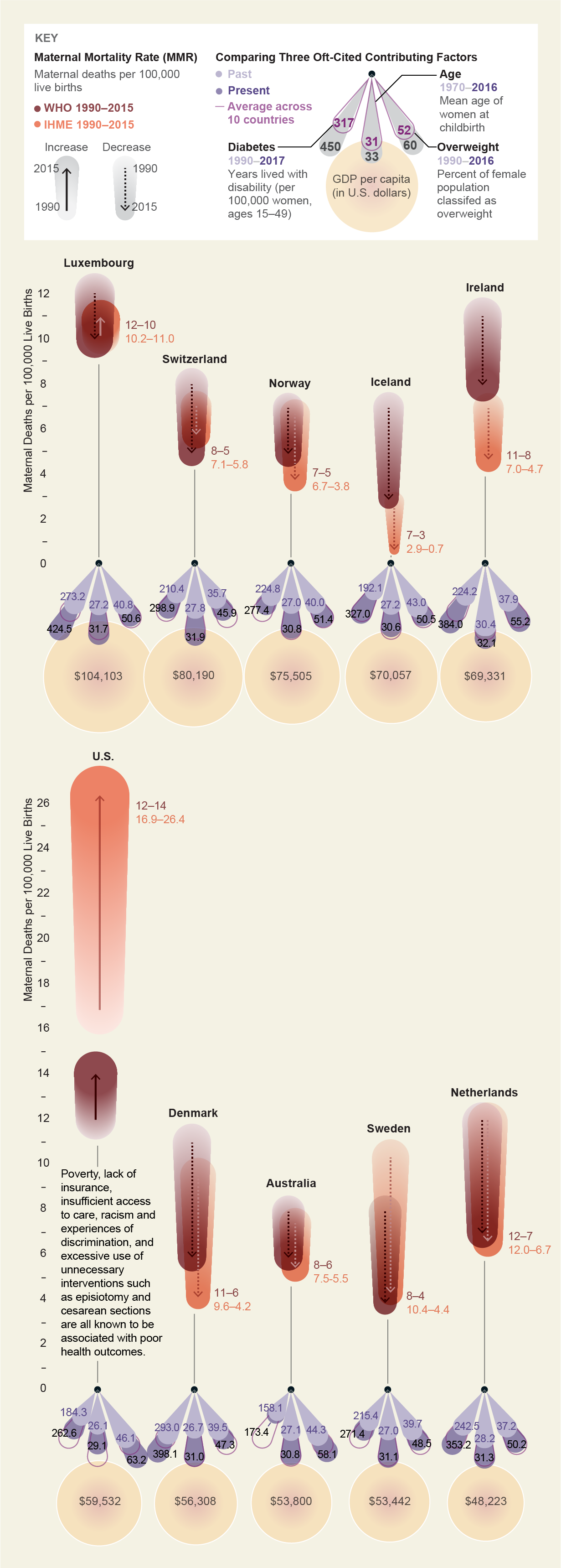
The U.S. Is an OutlierThe high maternal mortality rate (MMR) in the U.S. is often blamed on the poor health of mothers, but a comparison with other wealthy countries undermines this argument. MMR—shown here using two estimates, one by the World Health Organization (WHO) and one by the Institute for Health Metrics and Evaluation (IHME)—is not rising in countries with similarly increased rates of cardiovascular disease, obesity, diabetes and other conditions during pregnancy. Different factors must therefore be contributing to the rise in MMR in the U.S. As a 2018 paper in Obstetrics & Gynecology concluded, “the increased mortality ratios seen in the United States in recent years reflect significant social as well as medical challenges and are closely related to lack of access to health care in the non-Hispanic Black population.
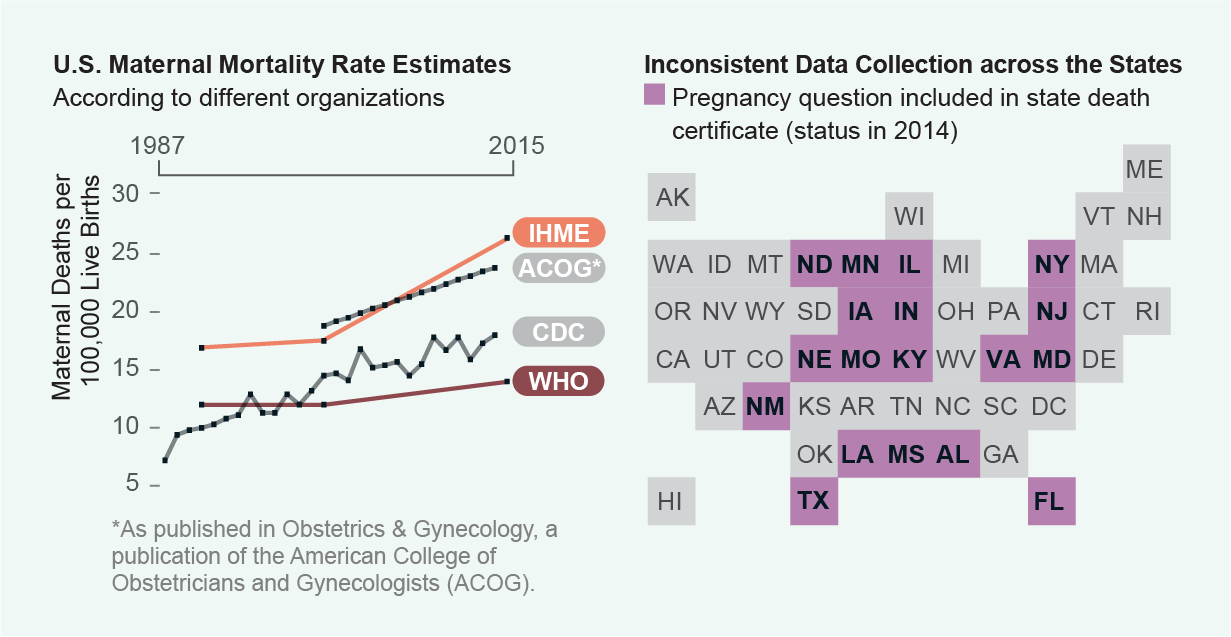
Maternal Mortality Data in the U.S. Are an Unreliable Mess
As bad as the numbers sound, the U.S. MMR is widely considered to be an underestimate. That is because different methods are used to count deaths related to pregnancy, and reporting is inconsistent. The World Health Organization, for instance, defines maternal death as the death of a woman while pregnant or within 42 days of the end of a pregnancy. But the Centers for Disease Control and Prevention defines maternal mortality as “the death of a woman while pregnant or within one year of the end of a pregnancy.” Both definitions exclude accidental or incidental causes of death. The difference in time frame for maternal mortality is further complicated at the state level, where data collection from death certificates is not comparable because of different definitions of the cause and time of death. States could fix this problem by creating standardized maternal mortality review committees that comprehensively evaluate each maternal death and discuss the factors that contributed to the outcome.
It’s common to blame women for their own deaths. Many scientific publications have cited that women are coming to pregnancy older (called advanced maternal age, or geriatric pregnancy), sicker (with hypertension, diabetes or other chronic illnesses) and fatter (that is, with obesity). But even in studies that control for age, chronic disease and obesity, the MMR in the U.S. still far exceeds rates in similarly wealthy nations. In a 2016 report that looked at pregnancy-related death disparities among states, the authors wrote that “excellent care is apparently available but is not reaching all the people.”
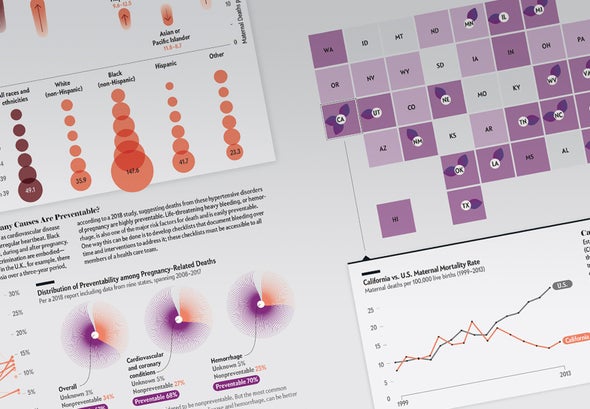
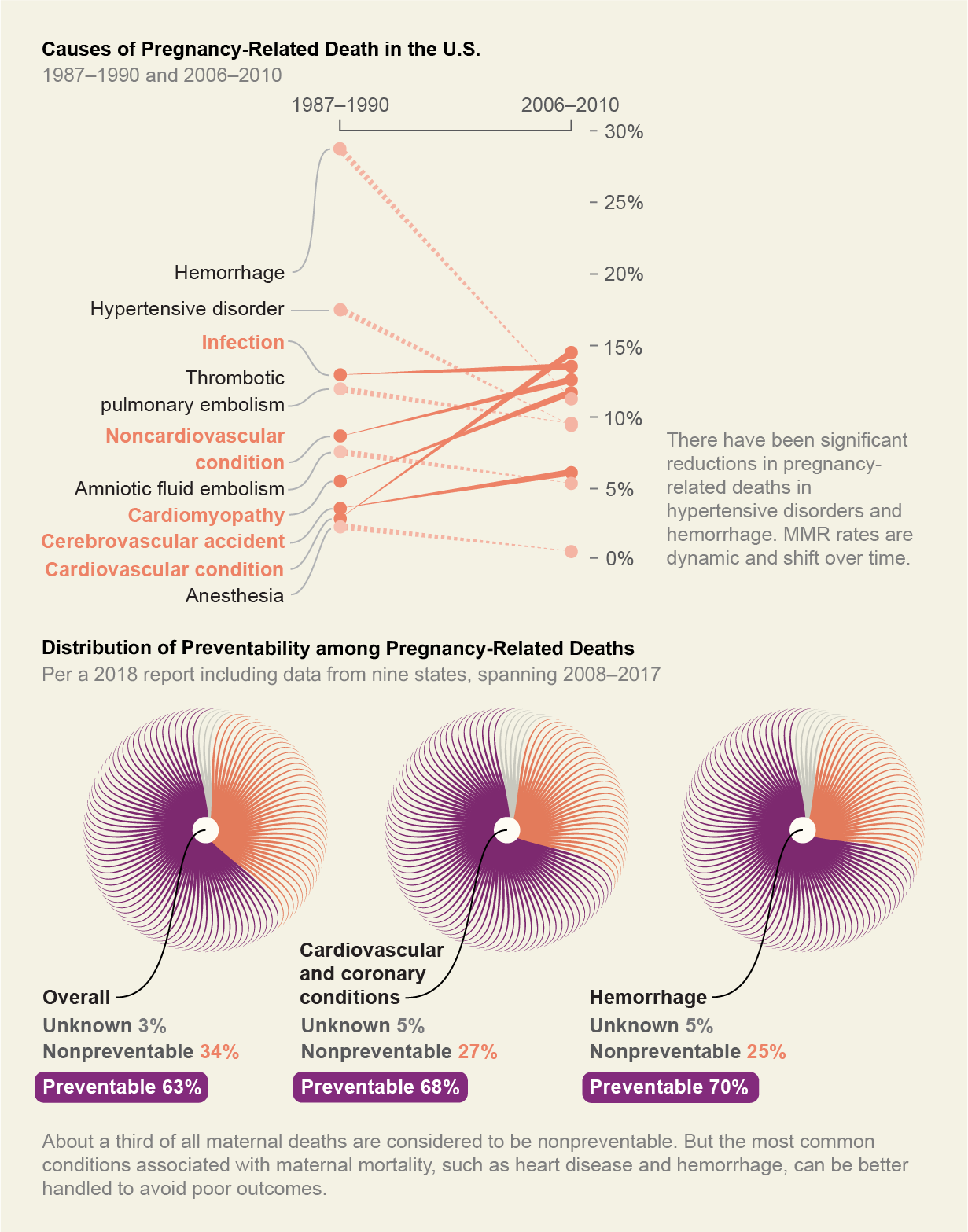
Why Are Mothers Dying—And How Many Causes Are Preventable?
Pregnancy exacerbates existing clinical conditions such as cardiovascular disease (including high blood pressure), enlarged heart and an irregular heartbeat. Black women are more likely to have these conditions before, during and after pregnancy. Chronic toxic stress—the way that experiences of discrimination are embodied—has been shown to make these conditions worse. But in the U.K., for example, there were only two deaths from preeclampsia and eclampsia over a three-year period, according to a 2018 study, suggesting deaths from these hypertensive disorders of pregnancy are highly preventable. Life-threatening heavy bleeding, or hemorrhage, is also one of the major risk factors for death and is easily preventable. One way this can be done is to develop checklists that document bleeding over time and interventions to address it; these checklists must be accessible to all members of a health-care team.
How the U.S. Is Tackling the Problem—Or Not
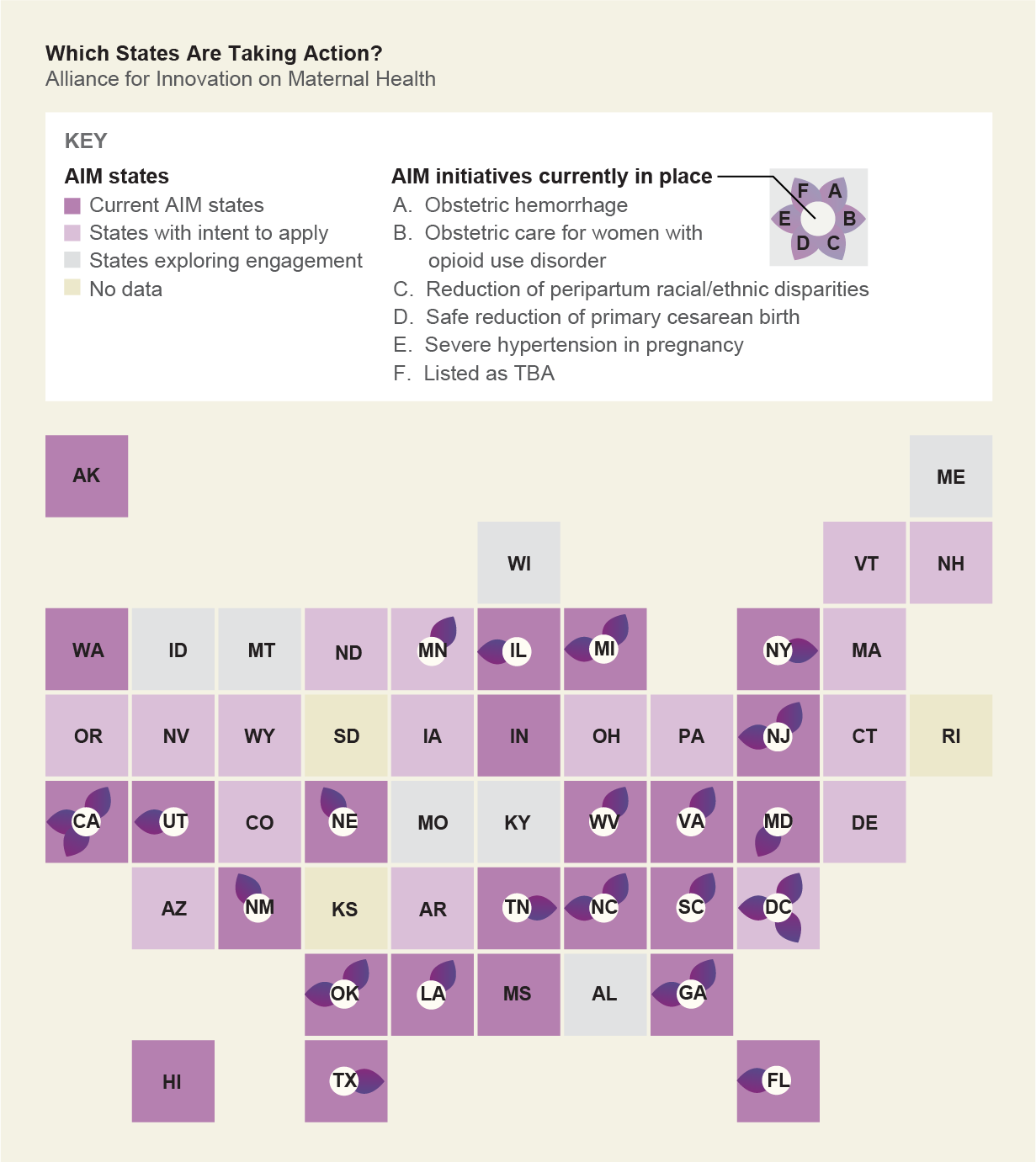
Several groups, including the World Health Organization, have called for a more respectful approach to maternal care. This would be helped by diversification of the health-care workforce so that clinical teams reflect the populations they serve. It also means better communication of knowledge between patients and their health-care teams. One program that embraces these features is called the Alliance for Innovation on Maternal Health (AIM). Funded through the federal Maternal and Child Health Bureau, AIM is a national alliance to promote consistent and safe maternity care. It launched with the initial goal of reducing maternal mortality by 1,000 instances—and severe maternal morbidity by 100,000 instances—between 2014 and 2018. Many states are currently participating. The efforts involved in AIM include hospital-based interventions whereby health-care teams—from obstetricians to emergency room staff—practice simulations of emergencies. The alliance also advocates for increased access to doulas and midwives, as well as a reclamation of normal physiological birth—that is, not treating birth as a disease to be managed.
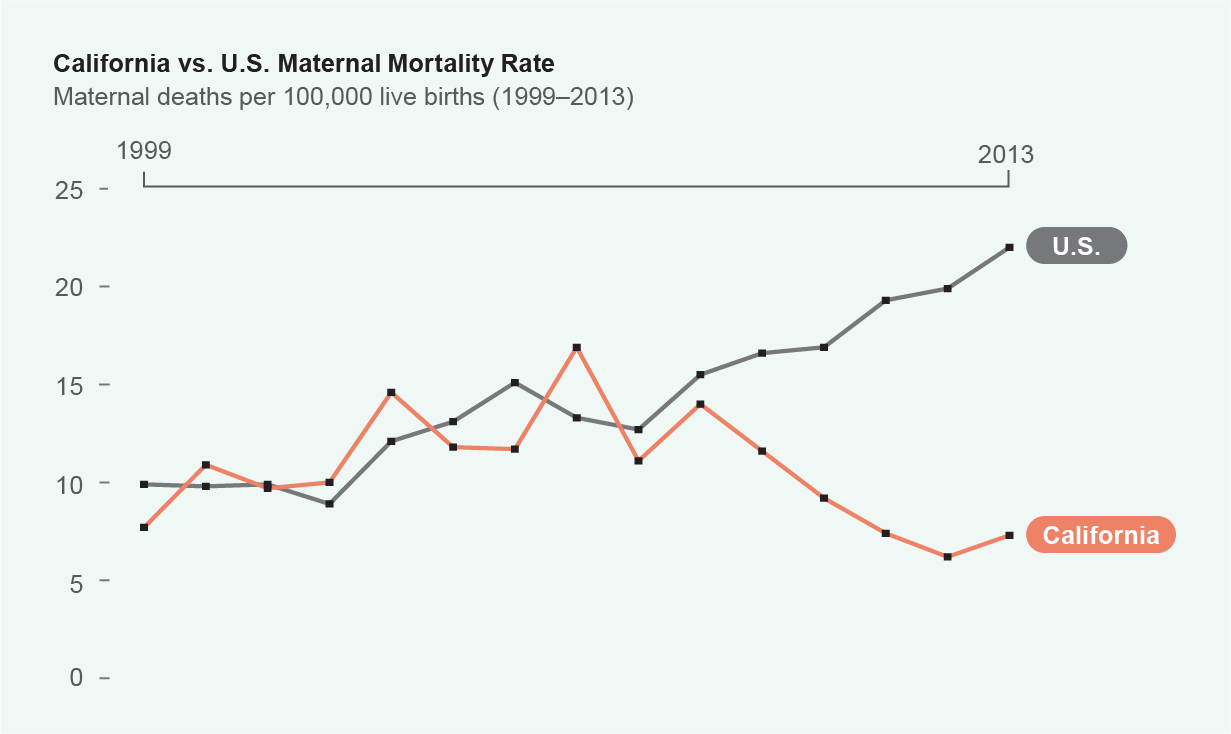
California Leads the Way
Established in 2006, the California Maternal Quality Care Collaborative (CMQCC) set out to use data-driven approaches to understand the root causes of maternal mortality. A few of their tactics included distributing plain-language tool kits, conducting mock emergencies, making quality improvements in hospital settings and training staff to work more collaboratively. Despite admirable reductions in overall maternal mortality in California, significant racial disparities remain and align with the demographics represented in the national data sets. Keeping Black women alive before, during and after birth was the focus of an innovative hospital-based racial equity pilot program: the SACRED Birth study, launched in 2020 by University of California, San Francisco, associate professor of obstetrics Karen A. Scott. This community-centered study co-led by Black women and community-based organizations provides essential insights on achieving birth equity and justice. Data collection ended at the beginning of 2021.
 Rights & Permissions
Rights & Permissions
