
The waiting room at the Mosaic Comprehensive Care Clinic in Chapel Hill, N.C., is as generic as any doctor's office except for a framed sign by the door. “No Wrong Way to Have a Body,” it says, above an illustration of different cacti species. The second anomaly of this primary care practice is what is missing from the exam rooms: there are no scales. Louise Metz, the clinic's owner and founder, keeps just one on the premises, tucked in a back hallway. Most patients never even know it is there.
Erin Towne, 37, who has come in for her annual physical, does know about the scale; she will stand on it during her examination so Metz can check whether she is continuing to restore her weight after recovering from a restrictive eating disorder. But only Metz will see the number. Towne, a mother of two who works in IT at a local university, is tall and slender, a runner. She wears a long sundress and hunches slightly as she sits in one of the exam room's armless chairs. The chairs are designed to support heavy people comfortably, and not so long ago Towne would have been grateful to see them. This willowy body is still relatively new to her. In January 2017 she underwent bariatric surgery, and she lost 160 pounds.
For most of her life, Towne says, “all of my health care has been focused on me losing weight.” After a series of blood sugar spikes at 13 years old, Towne was diagnosed with type 1 diabetes and started getting daily insulin injections. She was an average-sized kid, but her endocrinologist immediately suggested that she lose 10 to 15 pounds—a dictum that became the refrain of every doctor Towne saw as she grew older. It did not seem to matter that her diabetes was well controlled with a very low level of insulin; research dating back to the 1990s has shown an association between weight loss and better blood glucose management for diabetics, so weight-loss protocols are standard. Towne had been dieting since she was a teenager but never sustained the losses for long.
In 2016 Towne saw a new endocrinologist who changed her diagnosis to maturity-onset diabetes of the young, an inherited form of the condition. Even with an accurate diagnosis—and with confirmation that her diabetes was genetic in origin, not linked to weight—the obsession with making her smaller persisted, Towne says. Her doctor prescribed a diabetes medication called Victoza, which is also used for weight loss. Towne tried it for a month but experienced acid reflux so severe that she could not go to work. At that point bariatric surgery seemed inevitable. “I couldn't seem to keep the weight off any other way,” she says. “I had confidence that I could take care of my diabetes, but it seemed like no one else could split those two things apart.”
Within six months of her bariatric surgery, Towne's body mass index (BMI) had dropped to 19.1, which is at the low end of the “normal” range for a person her height. In May 2017 Towne was able to stop using her insulin pump, a victory her endocrinologist attributed to her weight loss. At a follow-up appointment in her surgeon's office in December 2017, a physician assistant seemed thrilled with the results. “Congratulations, you can eat extra cookies over the holidays!” Towne recalls the PA telling her. But Towne felt out of control around food. She had become obsessed with tracking exercise and calories on fitness apps. “I was restricting so intensely that my body was in emergency mode,” she says. “I would stand in front of my kitchen cabinets and picture myself eating everything in there.” A few weeks later Towne sought help from a therapist, who diagnosed her with anorexia and referred her to the Mosaic clinic for medical supervision during her recovery. Towne did not quite believe her therapist at first: “The idea that I had a restrictive eating disorder was mind-blowing,” she says. “I thought I was just doing what I'd always been told to do.”
Unlike Towne's previous doctors, Metz did not praise her patient's dramatic weight loss. In fact, Metz, an internal medicine physician, is suspicious of the long-held belief that weight loss is necessary for optimal diabetes care. “The studies that associate weight loss with improvements in A1C [a blood glucose measurement] are asking the wrong question,” she says. Weight may go down temporarily with a restrictive diet, but she believes that it is the changes in eating habits and exercise that cause the improvement, not the pounds lost. “And if those behavioral changes are too restrictive,” Metz adds, “they may make the problem worse.”
After taking Towne's history, Metz ordered an electrocardiogram—and then repeated it three times to confirm that Towne's resting heart rate had dropped into the low 50s, well below the normal range of 60 to 100 beats per minute. (Although low heart rates are considered healthy in endurance athletes, they are often a dangerous complication of severe weight loss and malnutrition, which can also cause arrhythmia and even death.) Metz also ran bloodwork, which revealed high cholesterol and estrogen that had dropped to menopausal levels, both of which are common side effects of anorexia. Metz showed her patient the test results and said, “None of this is okay.” It was a profoundly sobering moment for Towne. “My other doctors had never even noticed,” she says. “It was the first time I understood that my health was in more danger now that I was underweight than when I'd been at my highest weight.”
Questioning the Weight-Centric Model of Health Care
To Metz, Towne's lifelong health care experience is a classic example of how negative beliefs about high body weights lead to bias-informed medicine that hurts rather than heals. In Towne's case, her doctors' fixation on weight loss to manage her diabetes led them to miss other red flags and even to reinforce her disordered eating behaviors. In May 2018 a Canadian woman named Ellen Maud Bennett died only a few days after receiving a diagnosis of terminal cancer; in her obituary, her family wrote that Bennett had sought medical care for her symptoms for years but only ever received weight-loss advice. “We see this kind of stigma all the time in the typical medical visit when patients are shamed about their weight,” Metz says. “Assumptions are made about their health and lifestyle based on their size, and they often receive recommendations for weight loss rather than evidence-based treatments for their health conditions.”
Metz, who attended the University of North Carolina School of Medicine and did her residency in San Francisco before becoming an attending physician in New York, estimates that her first five to seven years as a doctor were spent in that same weight-centric mode.* “My private-practice patients all came in asking about weight loss, and I jumped right into it,” she says. Indeed, it is what the vast majority of health care providers have long assumed they should focus on since the early 20th century, when the life insurance industry began to collect data showing that a higher body weight predicted a shorter life span. In the 1970s physiologist Ancel Keys published research establishing a correlation between dietary fat and heart disease and proposed the modern BMI system, a measure of body fat based on weight and height that is used by many doctors to categorize health by weight.
By 1985 the National Institutes of Health had adopted the BMI as one of two official ways to assess body fat, and in 1998 an expert panel convened by the NIH put in place guidelines that moved 29 million Americans who had previously been classified as normal weight or just overweight into the overweight and obese categories. “This created the ‘obesity epidemic’ and really intensified the focus on weight as a risk factor for health,” says Jeffrey Hunger, an assistant professor of social psychology at Miami University in Oxford, Ohio, who studies health in stigmatized populations.
Defenders of the 1998 guidance say that research strongly supported the need for that shift and for medicine's increased and laserlike focus on weight as a health risk. “It is virtually incontrovertible that obesity has some negative impact,” says David Allison, dean and distinguished professor at the Indiana University-Bloomington School of Public Health. “It's pretty clear that it leads to elevated blood pressure and chronic inflammation, which both lead to problems.” But weight stigma (also known as weight bias), which is defined as the set of negative attitudes or beliefs that are expressed as stereotypes, prejudice and even overt discrimination toward people with higher-weight bodies, does harm, too. It can influence how scientists approach their research, leading to gaps in understanding of the relation between body size and health. It contributes to missed or delayed diagnoses and to chronic stress for patients. Meanwhile the medical community's goal of solving America's health problems by fixating on weight loss has proved nearly impossible to achieve.
Although the correlation between larger bodies and higher rates of heart disease, diabetes and other chronic conditions is well known, some of the mechanisms behind the relationship are not straightforward. Mainstream weight researchers argue that high body weight itself causes the elevated blood pressure and inflammation responsible for such conditions. Others, such as physiologist Lindo Bacon, say that the contribution of weight to health is complex and that the root cause of disease is more likely to be an intersection of the patient's genetics, life habits and environment.
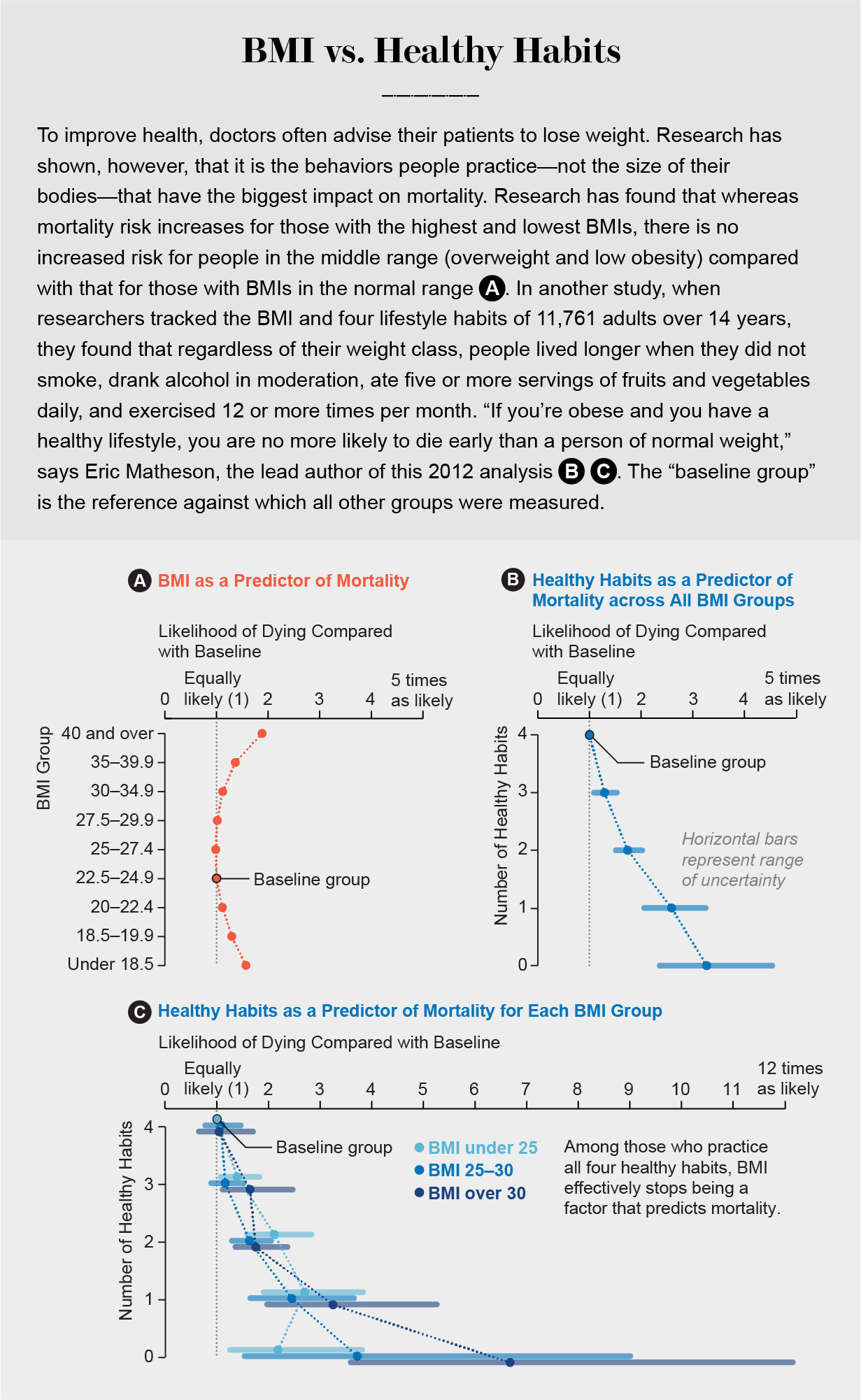
In some cases, data have shown that a higher body weight can actually be protective against certain health conditions. In the early 2000s researchers began noticing that heart surgery patients with higher BMIs had better survival rates than their thinner counterparts; this phenomenon was dubbed the “obesity paradox” and has also been documented for patients with osteoporosis (in whom higher body weight is thought to improve bone mineral density), major injuries and some kinds of cancer. The fact that a higher body weight actually helps people survive certain major illnesses could partially explain why individuals in overweight and low-obese BMI categories have an overall lower mortality risk according to the large epidemiology analyses of body weight and mortality correlations in the National Health and Nutrition Examination Survey (NHANES), the first of which was published by scientists at the Centers for Disease Control and Prevention in 2005. This research documents a “J curve” for the relation between BMI levels and mortality, meaning that whereas mortality risk increases for those with the highest and lowest BMIs, there is no increased risk for people in the middle range—overweight and low obesity—compared with that for those with BMIs in the normal range.
“The nadir of that J-shaped curve is getting higher on the BMI scale as we track populations over time,” explains Allison, who has studied the “obesity paradox.” “It could be that we have better treatments, so obesity doesn't kill you as quickly as it used to.” But the very fact that these findings are marveled over and classified as a paradox underscores the role of weight bias in how we think about weight and health, stigma researchers say. “A paradox is something contradictory or seemingly absurd,” Hunger notes. “This term only exists because it's considered absurd that fat people could actually be healthy.”
Scientific understanding of weight and health developed in tandem with cultural biases about body size, leading to a belief that weight is a matter of personal responsibility and willpower. Numerous studies dating back to about 1960 have documented how children, when shown pictures of kids with various body types, will nearly always rate the fat child as the one they like least. In a 1980 experiment, a public health researcher named William DeJong found that high school students shown a photograph of a higher-weight girl rated her as lazier and less self-disciplined than a normal-weight subject unless they were told her weight was caused by a thyroid condition. “Unless the obese can provide an ‘excuse’ for their weight ... or can offer evidence of successful weight loss, their character will be impugned,” he wrote.
DeJong's and others' early findings of weight stigma were regularly dismissed by mainstream researchers and health care providers alike. Then, in the early 2000s, a wealthy donor named Leslie Rudd, who had made his fortune in the food and beverage industry, approached a group of weight researchers at the Yale School of Medicine and asked them to study the impact of this stigma on people in larger bodies. “I was once a lot more overweight than I am now, and it gave me a firsthand insight into what people who are overweight feel and the discrimination they face,” Rudd was quoted as saying in a 2006 Yale press release. “There was very little work happening in this area,” says Kelly Brownell, a professor of public policy at Duke University and a former director of what became the Rudd Center for Food Policy and Obesity. Rebecca Puhl, then a graduate student of Brownell's, volunteered to lead the effort. “Basically, Rebecca created this field,” Brownell says. “And we were pretty quickly dumbfounded by what we found.”
Today ample evidence documents how people with larger bodies experience bias not only in health care settings but also in their workplaces, their schools and the media. Puhl, who is now deputy director for the Rudd Center at the University of Connecticut, and other scientists are beginning to show how living with this kind of chronic internal and external weight stigma negatively affects physical and mental health. This past March, Puhl and 35 of her colleagues released a consensus statement in the journal Nature Medicine condemning weight stigma as “inconsistent with current scientific evidence demonstrating that body weight regulation is not entirely under volitional control and that biological, genetic and environmental factors critically contribute to obesity.” They also issued a pledge, signed by more than 100 medical and scientific organizations, including the American Diabetes Association, to eradicate weight stigma by treating “individuals with overweight and obesity with dignity and respect,” especially in the workplace and in education and health care settings.
Yet weight loss continues to be promoted as a medical necessity for reducing mortality and managing chronic conditions such as heart disease and diabetes. That is why a small but growing group of weight researchers is pushing to replace the weight-centric model of health care with a “weight-inclusive” approach being pioneered by Metz and a handful of other medical practitioners around the country. Doctors who have embraced this strategy evaluate a patient's health and medical needs on the basis of blood pressure, cholesterol and other biomarkers, and they focus on the health benefits that can be reaped from improving behaviors related to diet and exercise regardless of whether such changes lower body weight. These factors may be more useful benchmarks for achieving healthy outcomes than BMI. A handful of randomized clinical trials and epidemiological studies have shown that improvements in diet and exercise habits can lower blood pressure and make other physiological gains even when study subjects do not lose weight, as Bacon and weight science researcher Lucy Aphramor concluded in their 2011 evidence review in Nutrition Journal. “What we're really doing is looking at patients as complex human beings rather than funneling all of our health concerns through their weight,” Metz explains. “We're stepping back to look at how the different organs and bodily systems interact with each other and then how a patient's environment, and even society as a whole, impacts their health.” If that approach could lead to healthier outcomes, would the medical and weight-science communities be ready to let go of the number on the scale?
How Weight Stigma Harms
Negative associations with large body types appear to cause real harm in health care settings. Kimberly Gudzune, an associate professor at the Johns Hopkins School of Medicine, has found that people who have been stigmatized for their weight in a doctor's office are less likely to come back. After analyzing audio recordings of 208 patient encounters with 39 primary care physicians, Gudzune found that doctors established less emotional rapport with their higher-weight patients, according to a study published in 2013 in the journal Obesity. In another paper, published in 2014, she found that 21 percent of patients with overweight and obese BMIs felt that their doctor “judged them about their weight”—and as a result, they were significantly less likely to trust their doctor.
This distrust appears to occur regardless of a patient's socioeconomic status. In one 2006 study, 68 percent of high-weight women reported that they had delayed seeking health care because of their weight, even though more than 90 percent of the study participants had health insurance. Gudzune says she observes this clinically all the time: “It's not unusual for me to see a patient who hasn't been to the doctor in 10 years, and now I'm telling them they have diabetes or hypertension. Who knows how many of those issues could have been prevented or at least better managed with earlier care?”

Even when patients with large bodies do continue to seek medical care, their provider's weight bias can compromise the quality of the care they receive. “Think about all the stereotypes we have that people with higher body weights are lazy, lack willpower and are uninterested in their own health,” Hunger says. “If that's the lens you walk in with to a clinical encounter, of course it shapes the questions you ask and the attitudes you take toward your patients.” Studies show that clinicians may be less willing to provide standard care to patients with high BMIs. In one survey of 1,316 physicians, 17 percent said they were reluctant to perform pelvic exams on patients with obese BMIs. In a 2011 study on patients reporting shortness of breath and several other ailments, medical students tended to prescribe weight-loss strategies rather than symptom management to patients with larger bodies.
Metz says she first became aware of the prevalence of weight stigma in health care 12 years ago while working in a primary care practice at Duke. She knew that when she treated patients with eating disorders, it was critical to avoid weigh-ins or discussions of weight-loss strategies because any focus on body size could trigger their deeply internalized shame and their propensity toward disordered eating and other destructive behaviors. “But then I'd leave that patient and walk next door to see someone who didn't have a diagnosed eating disorder but really wanted me to help them lose weight,” she recalls. Metz could not reconcile the disconnect she felt talking about portion control and calorie counting with larger patients—many of whom were dieting and exercising in extreme ways—when those same behaviors would be cause for concern in her thinner patients.
In fact, research suggests that restrictive eating disorders may be more prevalent in people with larger bodies. Classic anorexia nervosa is diagnosed in just 0.6 percent of Americans, perhaps in part because one of its diagnostic criteria is that patients must have reached an “extremely low body weight.” But atypical anorexia, which was added in 2013 to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders, is now used to diagnose patients who would otherwise meet criteria for anorexia but are not underweight; by one recent estimate, 2.8 percent of Americans would qualify for this diagnosis. Other research on eating disorders suggests that patients who develop them at higher weights are as much at risk for medical complications such as dangerously low blood pressure and slow heart rates as thinner patients, and they often struggle longer before receiving treatment, probably because doctors ignore or misdiagnose their symptoms. “It wasn't promoting my patients' health to prescribe weight loss,” Metz says. “It was doing harm.”
The harm caused by weight stigma appears to go well beyond misdiagnosis. A 2016 analysis of data collected from more than 21,000 American adults in the National Epidemiologic Survey on Alcohol and Related Conditions found a significant association between a person's experience of weight stigma and an increased incidence of heart disease, stomach ulcers, diabetes and high cholesterol even after researchers controlled for their subjects' socioeconomic status, physical activity level and BMI.
Puhl and other weight-stigma researchers have conducted experimental studies that have shown that people randomly assigned to “weight-stigma stimuli” consistently have higher physiological stress responses, such as increased cortisol levels, than those assigned to nonstigmatizing experiences. (One study by psychologists at Rutgers University and the University of California, Los Angeles, involved a researcher telling unwitting volunteers that they could not participate in an exclusive shopping experience, because they were too big and might stretch out the clothes.) These data suggest that weight stigma may be more than just unpleasant to live with; it might actually contribute to some portion of the poor health outcomes disproportionately seen in people with higher-weight bodies. “We know that physiological stress plays a role in body weight because higher levels of cortisol contribute to weight gain,” Puhl explains. “Weight stigma is a form of chronic stress. So that has chronic health effects, both physiologically and in terms of how people cope with that stress.”
If weight stigma can influence health directly by raising cortisol levels and blood pressure and indirectly by compromising the quality of care that patients with large bodies receive from their weight-biased doctors, is it possible that people with large bodies have worse health not just because of their literal size but also because of the way they are treated by the world for being that size? “Yes,” Brownell says without hesitation. He does not dispute the evidence for biological pathways between weight and health. “Obesity causes changes in the body that in turn increase risk factors, which in turn lead to diseases,” he explains. “But there are other pathways. And every pathway is exacerbated by the presence of weight stigma.”
Letting Go of the Scale Is Hard for Everyone
At the Mosaic Clinic, Leslie Scott, a 50-year-old woman who is in for her physical, still wants to be weighed. It is what she is used to, she says with a shrug. The medical tech obliges, but Metz does not look at the number before the checkup. She is more concerned about her patient's mental health. During her last visit, Scott mentioned that it was difficult to juggle work and being the primary caregiver for her elderly mother. Today Scott says her brother recently died and that she has been feeling depressed.
Metz closes her laptop and scoots her stool closer to her patient. “I'm so sorry,” she says. “That's a terrible loss.” They talk for several minutes about Scott's symptoms, such as how she is struggling to sleep and to remember to eat meals. “I know I need to take better care of myself,” Scott says. “I should probably start going back to the gym and walking more.”
“Do you enjoy those activities?” Metz asks. “And is it doable with your busy schedule, even once or twice a week?” Scott thinks it might be. Metz moves on to review Scott's vitals; her blood pressure is slightly elevated. “This is not in a range where you need medication, but it's something we'll watch,” she tells Scott.
“I think it's my diet and my weight,” Scott says. “It used to be high a few years ago. Then I lost weight, but now I've gained it back.”
Metz pauses. She chooses her next words carefully, making sure to avoid any hint of criticism of Scott or her previous doctors. “We hear a lot in health care settings that weight loss itself treats conditions like blood pressure,” she says. What the medical literature really shows, Metz continues, is it is not necessarily weight loss that helps; more likely, it is how our behavior changes. “So, I wonder: The time before, when your blood pressure got better, did you start to engage in different behaviors?”
“Well,” Scott says. “I moved away from a stressful situation.” Previously she worked 12-hour night shifts at the local jail; when she began a less dangerous day security job, “my blood pressure got worlds better.”
Metz senses an opening. These are the moments when patients often begin to connect the dots themselves and see how fixating so entirely on their weight has gotten in the way of larger health goals. At another medical practice, Metz worries, Scott's body size might have made her depression all too easy to miss. When her blood pressure rose before, nobody asked Scott about her job or her eating habits, let alone her mental health as she struggled to balance night shifts with the pressure of raising three children alone. “It was always just, ‘If you lose that weight, you won't have to take medication,’” Scott says.
Metz explains how the stress, lack of sleep and irregular eating habits caused by Scott's old job probably contributed to her previous hypertension. Then she notes how, in the months since her brother's death, Scott has begun struggling again with those same issues, albeit for different reasons. They talk through a plan to start managing Scott's depression with a combination of medication, counseling and some modest physical activity goals. Weight talk is off the table. “My concern for you right now is: Are you eating enough?” Metz says. Scott nods and laughs.
Even when doctors such as Metz want to offer an alternative to the weight-centric model of health care, they are often contending with patients who expect a weight-loss prescription. Yet weight is a trait that is far less mutable than experts have long thought. In the journal American Psychologist, an evidence review on the effectiveness of weight-loss interventions found that regardless of which diet people followed, they could lose some weight in the first nine to 12 months of any protocol, but over the next two to five years they gained back all but an average of 2.1 pounds. Nondieting control groups also gained weight during that time, though just 1.2 pounds on average. “The dieters had little benefit to show for their efforts, and the nondieters didn't seem harmed by their lack of effort,” says Traci Mann, one of the paper's co-authors, who is now a professor of psychology at the University of Minnesota. “Weight regain appears to be the typical response to dieting, not the exception.” Brownell, who studied public policy approaches to obesity prevention during his time at the Rudd Center, agrees that the data on its efficacy and durability are “too discouraging,” both because people struggle so much to lose and because their cycling between loss and subsequent weight regains seem to further elevate their risk for health issues.
Indeed, Dana Sturtevant, a registered dietitian, spent seven years managing weight-loss interventions in clinical trials comparing treatment protocols for hypertension. “Everybody on our trials did the same six-month curriculum, and they did lose some weight in those six months,” she recalls. “But they were always back up to where they started, or higher, at our two-year follow-up. When I'd bring that up in meetings, the researchers would say, ‘Well, it's the participants’ fault for not adhering to our protocol.'” It never occurred to her colleagues to question that protocol or whether weight loss should be the goal in the first place. Sturtevant began to “feel unethical” about her work; today she co-owns an organization called Be Nourished that teaches health care providers how to offer trauma-informed and weight-inclusive care. “We have no evidence-based treatment for high body weight that leads to sustained outcomes,” Sturtevant says. “If a medication had this kind of failure rate, doctors would stop prescribing it.”
Metz laments that there are only a handful of studies that compare weight-inclusive or “nondiet” treatments with weight-loss protocols. A 2005 study randomly assigned 78 women with obesity to either a diet protocol or a Health at Every Size intervention. For the latter, participants were counseled about body acceptance, encouraged to separate their self-worth from their weight, and educated about techniques for intuitive eating and strategies for finding physical activity they enjoyed. The dieters lost weight but regained it; they were more likely to quit the program and saw fewer overall improvements in health outcomes than those using the nondiet intervention. A 2018 study found that following a similar Health at Every Size protocol helped participants improve their psychological well-being, physical stamina and overall quality of life even though they did not lose weight. Such results are encouraging, but Metz says more data are needed to understand and fine-tune the approach.
One such piece of research, which Metz refers to often, is a 2012 analysis of the NHANES data published by Eric Matheson, an associate professor of family medicine at the Medical University of South Carolina, and his colleagues. They found that life habits were a strong predictor of mortality because regardless of their weight class, people lived longer when they practiced healthy habits such as not smoking, drinking alcohol in moderation, eating five or more servings of fruits and vegetables daily, and exercising 12 or more times a month. “If you're obese and you have a healthy lifestyle, you are no more likely to die early than a person of normal weight,” Matheson says.
Some discrepancies exist in his data; for example, eating more vegetables was associated with lower mortality for folks in the normal and overweight categories but not for obese people, whereas exercising regularly appeared to help those in the normal and obese groups but not people in the overweight range. Matheson does not know how to explain those findings. But one possible explanation is that the weight classifications themselves are somewhat arbitrary, something that even the mainstream weight researchers acknowledge. “At every level of the BMI, people can have different degrees of body fat or be that size because of entirely different factors or combinations of factors,” Allison says. “Their age, race, sex and genetic background all come into play when we try to say whether their level of adiposity will cause health effects. It's not as simple as saying obesity is bad. You have to know for what, for whom, for when.”
Metz is not sure that she has figured out the best approach to health care, but she sees patients every day who affirm that she is evolving in the right direction. Midway through her physical, Towne mentions that she has recently been discharged from eating-disorder therapy. “That's wonderful!” says Metz, breaking into a warm smile. They talk a little more about Towne's diet as Metz thoughtfully frames the conversation, asking, “Does your body give you feedback after you eat that?” instead of offering prescriptive advice about what to eat or avoid, as a different doctor might have. One risk of the weight-inclusive model is that conversations about “healthy habits” can still easily turn into more opportunities to judge patients for their ability to comply with doctor's orders; talking about portion control and “lifestyle changes” can come across as a coded way of encouraging weight loss. But Metz is determined to push only changes that are sustainable for her patients and that have clear benefits regardless of whether they lead to weight loss.
Towne tells me later that one of the biggest challenges of recovering from her eating disorder has been accepting that her weight is not something she needs to control. “I don't know if I'll stay in a smaller body. And that's complicated because I have a lot of leftover trauma around how I was treated as a bigger person,” she says. But Metz helped her see that fixating on being small, rather than healthy, had led to serious medical ramifications. “Having a doctor who can so totally remove weight from my health care has been literally life-changing.”
*Editor‘s Note (6/24/20): This sentence has been edited after posting to correct a reference to the medical school Louise Metz attended.
 Rights & Permissions
Rights & Permissions
