
In 2018, psychiatrist Oleguer Plana-Ripoll was wrestling with a puzzling fact about mental disorders. He knew that many individuals have multiple conditions—anxiety and depression, say, or schizophrenia and bipolar disorder. He wanted to know how common it was to have more than one diagnosis, so he got his hands on a database containing the medical details of around 5.9 million Danish citizens.
He was taken aback by what he found. Every single mental disorder predisposed the patient to every other mental disorder—no matter how distinct the symptoms. “We knew that comorbidity was important, but we didn’t expect to find associations for all pairs,” says Plana-Ripoll, who is based at Aarhus University in Denmark.
The study tackles a fundamental question that has bothered researchers for more than a century. What are the roots of mental illness?
In the hope of finding an answer, scientists have piled up an enormous amount of data over the past decade, through studies of genes, brain activity and neuroanatomy. They have found evidence that many of the same genes underlie seemingly distinct disorders, such as schizophrenia and autism, and that changes in the brain’s decision-making systems could be involved in many conditions.
Researchers are also drastically rethinking theories of how our brains go wrong. The idea that mental illness can be classified into distinct, discrete categories such as ‘anxiety’ or ‘psychosis’ has been disproved to a large extent. Instead, disorders shade into each other, and there are no hard dividing lines—as Plana-Ripoll’s study so clearly demonstrated.
Now, researchers are trying to understand the biology that underlies this spectrum of psychopathology.
They have a few theories. Perhaps there are several dimensions of mental illness—so, depending on how a person scores on each dimension, they might be more prone to some disorders than to others. An alternative, more radical idea is that there is a single factor that makes people prone to mental illness in general: which disorder they develop is then determined by other factors. Both ideas are being taken seriously, although the concept of multiple dimensions is more widely accepted by researchers.
The details are still fuzzy, but most psychiatrists agree that one thing is clear: the old system of categorizing mental disorders into neat boxes does not work. They are also hopeful that, in the long run, replacing this framework with one that is grounded in biology will lead to new drugs and treatments. Researchers aim to reveal, for instance, the key genes, brain regions and neurological processes involved in psychopathology, and target them with therapies. Although it might take a while to get there, says Steven Hyman of the Broad Institute of MIT and Harvard in Cambridge, Massachusetts, “I am long-term optimistic if the field really does its work.”
A smorgasbord of disorders
The most immediate challenge is working out how to diagnose people. Since the 1950s, psychiatrists have used an exhaustive volume called the Diagnostic and Statistical Manual of Mental Disorders, currently in its fifth edition. It lists all the recognized disorders, from autism and obsessive–compulsive disorder to depression, anxiety and schizophrenia. Each is defined by symptoms. The inherent assumption is that each disorder is distinct, and arises for different reasons.
However, even before the DSM-5 was published in 2013, many researchers argued that this approach was flawed. “Any clinician could have told you that patients had not read the DSM and didn’t conform to the DSM,” says Hyman, who helped to draft the manual’s fifth edition.
Few patients fit into each neat set of criteria. Instead, people often have a mix of symptoms from different disorders. Even if someone has a fairly clear diagnosis of depression, they often have symptoms of another disorder such as anxiety. “If you have one disorder, you’re much more likely to have another,” says Ted Satterthwaite, a neuropsychiatrist at the University of Pennsylvania in Philadelphia.
This implies that the way clinicians have partitioned mental disorders is wrong. Psychiatrists have tried to solve this by splitting disorders into ever-finer subtypes. “If you look at the way the DSM has evolved over time, the book gets thicker and thicker,” says Satterthwaite. But the problem persists—the subtypes are still a poor reflection of the clusters of symptoms that many patients have.
As a result, the world’s largest funder of mental-health science, the US National Institute of Mental Health, changed the way it funded research. Beginning in 2011, it began demanding more studies of the biological basis of disorders, instead of their symptoms, under a programme called the Research Domain Criteria. There has since been an explosion of research into the biological basis of psychopathology, with studies focusing on genetics and neuroanatomy, among other fields. But if researchers hoped to demystify psychopathology, they still have a long way to go: the key finding has been just how complex psychopathology really is.
Controversial clusters
Clinically, the evidence that symptoms cut across disorders—or that people frequently have more than one disorder—has only grown stronger. For this reason, although individual symptoms such as mood alterations or impairments in reasoning can be diagnosed reliably, assigning patients to an overall diagnosis such as ‘bipolar disorder’ is difficult.
Even seemingly separate disorders are linked. In 2008, geneticist Angelica Ronald, then at King’s College London Institute of Psychiatry, and her colleagues found that autism and attention deficit hyperactivity disorder (ADHD) overlapped. “At the time, you weren’t allowed to be diagnosed with both conditions,” says Ronald; this was because of a rule in an earlier version of the DSM. But she and her team found that traits for autism and ADHD were strongly correlated, and partially under genetic control.
Furthermore, there seem to be clusters of symptoms that cross the boundaries of disorders. A 2018 study examined people who had been diagnosed with either major depression, panic disorder or post-traumatic stress disorder (PTSD). The volunteers were assessed on the basis of their symptoms, cognitive performance and brain activity. The researchers found that the participants fell into six groups, characterized by distinct moods such as ‘tension’ and ‘melancholia’. The groups cut across the three diagnostic categories as if they were not there.
Many now agree that the diagnostic categories are wrong. The question is, with biology as their guide, what should psychiatric diagnosis and treatment look like instead?
Multiple dimensions
One prominent model is that there are a number of neuropsychological traits or ‘dimensions’ that vary in every person. Each trait determines our susceptibility to certain kinds of disorder. For example, someone might be prone to mood disorders such as anxiety, but not to thought disorders such as schizophrenia.
This is similar to the way psychologists think about personality. In one model, five personality traits, such as conscientiousness and neuroticism, describe most of the variation in human personalities.
Some psychiatrists are already trying to reimagine their discipline with dimensions in mind. In the early 2010s, there was a push to eliminate disorder categories from the DSM-5 in favour of a ‘dimensional’ approach based on individual symptoms. However, this attempt failed—partly because health-care funding and patient care has been built up around the DSM’s categories. However, other catalogues of disorders have shifted towards dimensionality. In 2019, the World Health Assembly endorsed the latest International Classification of Diseases (called ICD-11), in which some psychopathologies were newly broken down using dimensional symptoms rather than categories.
The challenge for the dimensionality hypothesis is obvious: how many dimensions are there, and what are they? Satterthwaite calls this “a very large problem”.

One popular theory, supported by many studies over the past decade, argues for just two dimensions. The first includes all ‘internalizing’ disorders, such as depression, in which the primary symptoms affect a person’s internal state. This is contrasted with ‘externalizing’ disorders, such as hyperactivity and antisocial behaviour, in which a person’s response to the world is affected. If someone has been diagnosed with two or more disorders, studies suggest these are likely to be from the same category.
But studies combining large amounts of brain-imaging data with machine learning have turned up different numbers—even in studies done by the same lab. Last year, Satterthwaite and his group published a study of 1,141 young people who had internalizing symptoms, and found they could be split into two groups on the basis of their brain structure and function. In 2018, Satterthwaite led a similar study and identified four dimensions, each associated with a distinct pattern of brain connectivity.
Ultimately, a future version of the DSM could have chapters devoted to each dimension, says Hyman. These could list the disorders that cluster within each, as well as their symptoms and any biomarkers derived from the underlying physiology and genetics. Two people who had similar symptoms but different sets of mutations or neuroanatomical alterations could then be diagnosed and treated differently.
In the genes
One pillar of this future approach is a better understanding of the genetics of mental illness. In the past decade, studies of psychopathological genetics have become large enough to draw robust conclusions.
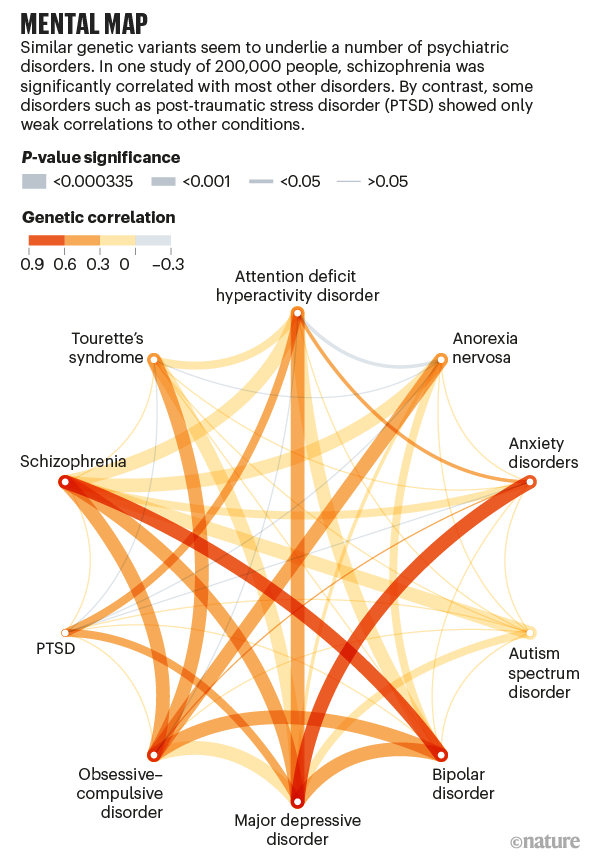
The studies reveal that no individual gene contributes much to the risk of a psychopathology; instead, hundreds of genes each have a small effect. A 2009 study found that thousands of gene variants were risk factors for schizophrenia. Many were also associated with bipolar disorder, suggesting that some genes contribute to both disorders.
This is not to say that the same genes are involved in all brain disorders: far from it. A team led by geneticist Benjamin Neale at Massachusetts General Hospital in Boston and psychiatrist Aiden Corvin at Trinity College Dublin found in 2018 that neurological disorders such as epilepsy and multiple sclerosis are genetically distinct from psychiatric disorders such as schizophrenia and depression.
These studies all looked at common variants, which are the easiest to detect. Some recent studies focused instead on extremely rare variants, which do suggest genetic differences between disorders. A study of more than 12,000 people found that individuals with schizophrenia had an unusually high rate of ultra-rare mutations—and that these were often unique to one individual.
The result is a mess. It is difficult to predict which risk factors cut across conditions. “Some of them are quite broadly shared across psychopathology,” says Neale, “whereas some are a bit more specific to one or a handful of forms of psychopathology.”
The p factor
Some psychiatrists have put forward a radical hypothesis that they hope will allow them to make sense of the chaos. If disorders share symptoms, or co-occur, and if many genes are implicated in multiple disorders, then maybe there is a single factor that predisposes people to psychopathology.
The idea was first proposed in 2012 by public-health specialist Benjamin Lahey at the University of Chicago in Illinois. Lahey and his colleagues studied symptoms in 11 disorders. They used statistics to examine whether the pattern could best be explained by three distinct dimensions, or by those three together with a ‘general’ predisposition. The model worked better if the general factor was included.
The following year, the hypothesis received more support—and a catchy name—from husband-and-wife psychologists Avshalom Caspi and Terrie Moffitt at Duke University in Durham, North Carolina. They used data from a long-term study of 1,037 people and found that most of the variation in symptoms could be explained by a single factor. Caspi and Moffitt called this the ‘p factor’. Since 2013, multiple studies have replicated their core finding.
Caspi and Moffitt were clear that the p factor could not explain everything, and made no guesses about its underlying biology, speculating only that a set of genes might mediate it. Others have proposed that the p factor is a general predisposition to psychopathology, but that other factors—stressful experiences, or other gene alterations—nudge a person towards different symptoms. But if it is real, it has a startling implication: there could be a single therapeutic target for psychiatric disorders.
There are already hints that generalized treatments could work just as well as targeted therapies. A 2017 study randomly assigned people with anxiety disorders, such as panic disorder or obsessive–compulsive disorder, to receive either a therapy for their specific disorder or a generalized approach. Both therapies worked equally well.
Finding a physiological basis for the p factor would be the first step towards therapies based on it, but only in the past few years have researchers found hints of it in genetic and neuroanatomical data. One study of the genetics of psychopathology in a UK population, for instance, identified a ‘genetic p factor’—a set of genes in which there were variations that contributed to the risk of psychopathology.
Meanwhile, other groups have searched for a neuroanatomical change that occurs in multiple psychopathologies. The results are intriguing, but contradictory.
One study of six psychopathologies found that the brain’s grey matter shrank in three regions involved in processing emotions: the dorsal anterior cingulate, right insula and left insula. But subsequent studies by Adrienne Romer, a clinical psychologist now at Harvard Medical School and McLean Hospital in Belmont, Massachusetts, identified a totally different trio of regions with roles that include managing basic bodily functions and movement—the pons, cerebellum and part of the cortex. One key to making sense of this might be to focus on the brain’s executive function: the ability to regulate behaviour by planning, paying attention and resisting temptation, which relies on many brain regions. Romer and Satterthwaite have independently found disruptions in executive function in a range of psychopathologies—the suspicion being that these disruptions could underlie the p factor.
Most scientists agree that what is needed is more data, and many remain unconvinced by such simple explanations. “I’m a little less certain that that’s how it’s going to play out,” says Neale. At the genetic level at least, he says, there are many disorders, such as PTSD and generalized anxiety disorder, that remain poorly understood.
All such sweeping hypotheses are premature, says Hyman. “I think it’s a time for much more empirical research rather than grand theorization.”
This article is reproduced with permission and was first published on May 5 2020.
