
Even before the results of the 2016 presidential election were official, women on social media began offering a tip for surviving the next four years: get an IUD tomorrow.
Small, plastic T-shaped devices loaded with synthetic hormones or wrapped with copper coil, IUDs—or intrauterine devices—are inserted into the uterus to offer pregnancy prevention for years. Along with less frequently used hormonal implants that go in the arm, they are known in the reproductive health field as long-acting reversible contraception, or LARC. And with a new leader who pledged to repeal the Affordable Care Act, along with its mandate to cover contraception with no co-pays, many women figured they should seize the chance to secure long-lasting birth control while they still could.
Plenty heeded this advice. Shortly after the election, the president of Planned Parenthood said the organization had seen a “900 percent increase” in IUD-insertion appointments at its clinics nationwide. In March 2019 a study published in JAMA Internal Medicine confirmed that the number of women receiving LARC rose by 21.6 percent in the month after Donald Trump won the presidency.
While this so-called Trump bump was significant, the comeback of IUDs began several years earlier. In 2002 just 2 percent of U.S. women using contraception chose them. In 2014 that number rose to 11.8 percent, an all-time high that matches the average prevalence among other developed nations. For decades IUDs had a bad image after the Dalkon Shield, a poorly designed device from the 1970s, caused infections, infertility and even death in tens of thousands of women. Today’s models are much safer, and younger women don’t have the same negative associations with IUDs as prior generations. Before 2010 the high up-front cost of such a device—up to several hundred dollars—was often a nonstarter. But under the still intact Affordable Care Act, insertion is free with private health insurance.
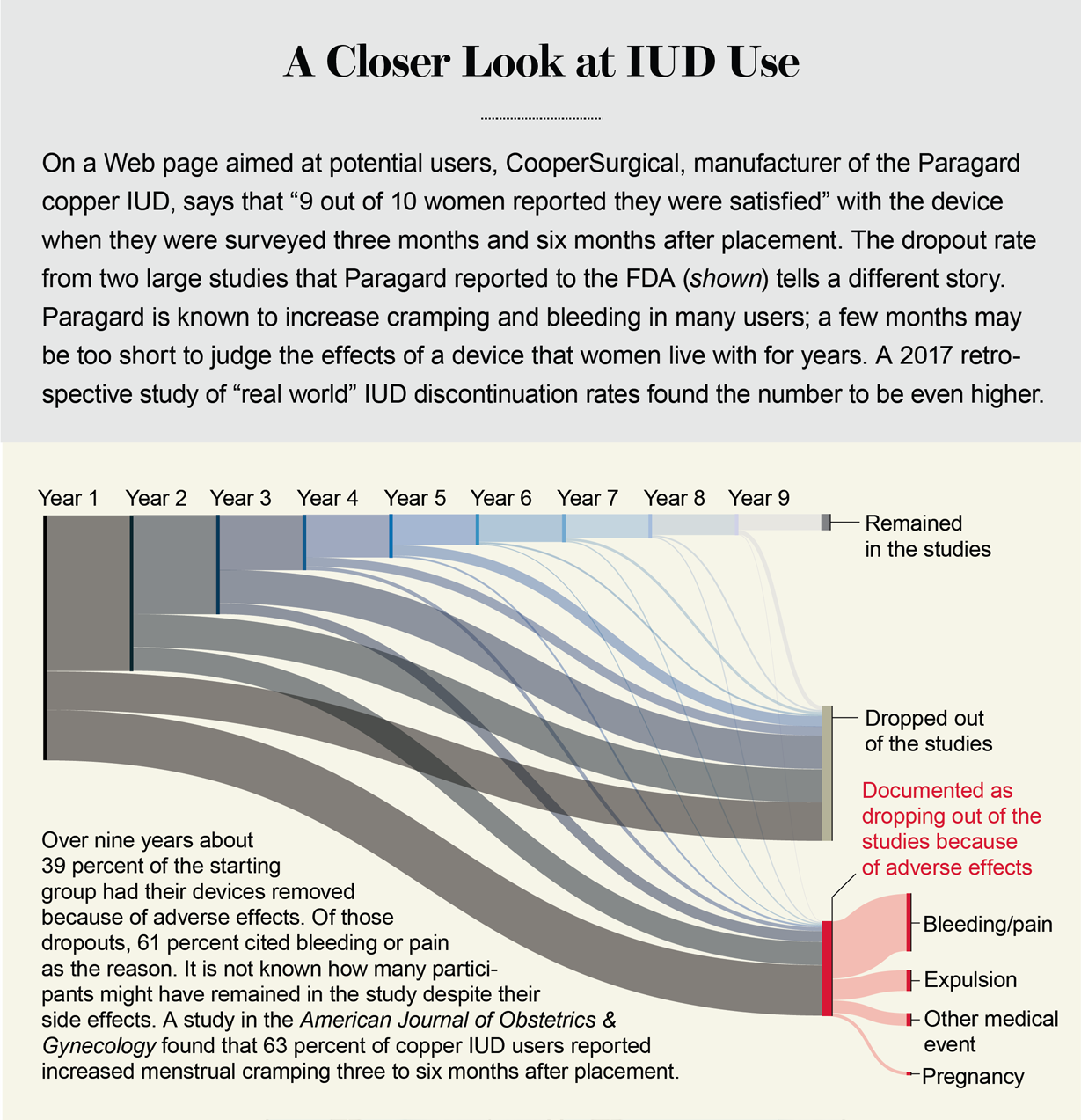
Credit: Amanda Montañez; Source: ParaGard® T380A Intrauterine Copper Contraceptive. Prescribing information. Teva Women’s Health. Submitted to Food and Drug Administration on June 11, 2013
IUDs have also benefited from a concerted advocacy effort to eliminate barriers to their use. A Colorado outreach initiative to provide low-income women with no-cost IUDs and implants, which was launched in 2009, led to significant declines in the state’s teen birth and abortion rates and drew national attention. Since 2014 a nonprofit called Upstream has offered training and technical assistance to health centers to increase same-day access to all forms of birth control, particularly LARC. Upstream currently partners with state governments in Delaware, Massachusetts, Washington State and North Carolina. Under the program, use of IUDs and implants among low-income women in Delaware more than doubled in three years. Forty states have now changed their Medicaid policies to reimburse hospitals for inserting IUDs in the delivery room immediately postpartum.
The rising popularity of the IUD represents the largest shift in American contraceptive trends in recent decades. Researchers at the Guttmacher Institute say it has contributed to an 18 percent decrease in the unintended pregnancy rate between 2008 and 2011: a “historic” low after a long period of stagnation. Both the American College of Obstetricians and Gynecologists (ACOG) and the American Academy of Pediatrics now recommend IUDs as a top birth-control option for all women, including adolescents.
It’s easy to see why IUDs are so appealing: less than 1 percent of users will get pregnant in a year, making the devices just as effective as sterilization, and they last between three and 12 years. What gives IUDs the most compelling edge over other methods is that they are practically immune to human error. Once inserted, you don’t have to do anything else—interrupt sex to put on a condom or remember to take a pill at the same time every day—to get reliable pregnancy prevention. It is this feature in particular that has led to a common refrain in the reproductive health field: “Set it and forget it,” an Upstream trainer recently told the New York Times, borrowing the advertising tagline of a rotisserie chicken oven to describe the IUD.
On the surface, this highly effective, long-acting, difficult-to-mess-up form of birth control seems to be well liked. ACOG’s guidelines point out that IUDs have the highest continuation rates and user satisfaction of all reversible birth-control methods. Diana Blithe, program director for contraception development at the National Institutes of Health’s National Institute of Child Health and Human Development (NICHD), says the introduction of the first hormonal IUD in 2000, in particular, “has been a bit of a game changer in that women like it.” Three fourths of IUD users in the U.S. choose a hormonal IUD (as opposed to the nonhormonal copper IUD), which tends to make menstrual periods lighter or disappear altogether. “It’s really effective and popular—it’s all good,” Blithe says.
There are plenty of self-described IUD evangelists. But that’s not the whole picture. Although IUDs do work well for many women, a significant number experience side effects and sometimes debilitating ones. As medical devices, IUDs have drawbacks that other contraceptive methods do not. Without easy access to a health care provider—and one who takes a patient’s symptoms seriously—“set it and forget it” can start to sound less like convenience and more like coercion.
The IUD cheerleading obscures a broader illusion of choice. Nearly 60 years after the first oral contraceptive pill was sold, most prescription birth-control methods are variations on the same synthetic hormones that have always been used. The first IUDs date back even further, to a time when inert devices made of silkworm gut or metal stopped pregnancy by creating sustained inflammation. At a time when lawmakers are constantly threatening to roll back access to all aspects of reproductive health care, it can feel risky to criticize birth-control methods. After all, ultraconservative foes of birth control tend to manipulate concerns about side effects and risks into a reason women should forgo contraception entirely. But in 2020 it is worth asking: Why don’t we have more innovative birth-control options? When it comes to preventing pregnancy, is a device that works in part by irritating the uterus really the best science can provide?
Measuring dissatisfaction
Much of the recent enthusiasm over IUDs can be traced back to a single study called the Contraceptive CHOICE research project. Funded in part by a then anonymous donor now known to be the Susan Thompson Buffett Foundation and facilitated by Washington University in St. Louis, the project had the explicit goal of increasing the use of LARC among women at high risk of unintended pregnancy.
Between 2007 and 2011 a cohort of 9,256 women and adolescent girls were offered their choice of a contraceptive method free of charge. Participants received “tiered contraceptive counseling,” in which they were presented with the risks and benefits of each method in order of most effective to least effective, meaning that they heard about IUDs and implants first. Three quarters of the participants chose to use those LARC methods, and those who did were 20 times less likely to have an unintended pregnancy than those who chose other prescription methods such as the pill.
In addition to this dramatic effect on unintended pregnancy rates, the reproductive health field was excited by the discontinuation rates found in the CHOICE study. The number of women who had their IUD or implant removed early was much lower, relative to the study participants who had abandoned their non-LARC methods. Remarkably, 69 percent of the women who had chosen oral contraceptives, injection, the vaginal ring or the skin patch had given up on them after three years—more than twice the dropout rate of the IUD users. As such, the IUD was held up as the form of birth control that users liked the most.
But what is often underdiscussed are the IUD discontinuation rates themselves. After one year nearly 20 percent of copper IUD users and about 14 percent of hormonal IUD users reported they were “not satisfied” with the device; 12.5 and 16 percent, respectively, had had it removed. Around the five-year mark, 44.1 percent of copper IUD—and 48.3 percent of hormonal IUD—users had discontinued the device. About two thirds of those who had done so by the end reported that the reason was because of pain, bleeding changes or other side effects or because the foreign object had been expelled from their body. In other words, the IUD dropout rate linked to side effects looks low largely in the context of other methods.
The CHOICE findings, which have been reported in nearly 70 published papers and more than 500 media outlets, helped to spur a shift in the field from “options-based” contraceptive counseling, in which a range of methods are presented, to the “LARC-first” counseling used in the CHOICE study. Even the ACOG guidelines cite the CHOICE study as evidence of the “superiority of LARC methods over short-acting methods.” Manufacturer brochures for IUDs, such as from CooperSurgical, manufacturer of Paragard, also use CHOICE data to promote their devices to women.
Other studies have reported markedly higher discontinuation rates. In the original Food and Drug Administration clinical trials, the five-year rates for the copper Paragard and hormonal Mirena were 60 percent and 55 percent, respectively. Then, in 2017, a retrospective study at Harvard Medical School of more than 1,000 American women found that at five years, 71.9 and 76.2 percent, respectively, had removed their device. The researchers suggested that these results might better reflect “real-world” rates in the clinical setting, “outside of the structured setting of a randomized controlled trial,” or the CHOICE study, which was trying to increase uptake of LARC and offered subjects “extensive counseling.”
That IUDs are comparatively well liked might say less about how popular they are and more about how dissatisfied women are with birth control in general. Perhaps the IUD is just the least onerous option out of an unimpressive field. According to an analysis of data from the 2006–2010 National Survey of Family Growth, women in the U.S. have tried a median of three contraceptive methods. Whereas many women eventually find one that works well for them—often after years of trial and error—some simply settle on one out of sheer frustration: nearly two fifths of women surveyed in 2004 by the Guttmacher Institute said they chose their current method mostly because they didn’t like any other available options.
It is hard to know what self-reported “satisfaction” is even measuring when it comes to contraception. “Many women tolerate negative side effects because their sense of the risk of pregnancy is higher or their anticipation of the consequence of a pregnancy is worse,” says Diana Greene Foster, director of research at Advancing New Standards in Reproductive Health (ANSIRH) at the University of California, San Francisco. Nearly 40 percent of women in the Guttmacher survey said they were not satisfied with the method they were currently using. And that makes them less likely to use it consistently. For example, 48 percent of dissatisfied oral contraceptive users skipped at least one pill in the past three months as compared with 35 percent of satisfied users.
Just how far we are from having a variety of options that truly meet women’s needs becomes clear when you ask them what they actually want in a contraception method, which Foster and her colleagues did in a 2012 study. The three features deemed “extremely important” by the largest proportions of women were effectiveness (84 percent), lack of side effects (78 percent) and affordability (76 percent). Then they determined how many of the currently available methods met the women’s criteria and found that “for 91 percent of women, no contraceptive method has all the features they think are extremely important.” Perhaps unsurprisingly, what women really want is a highly effective method with few or no side effects. And as the researchers explain in the study, “that combination does not exist.”
The IUD discontinuation rates seem more notable after considering how much harder it is to stop using a device that is lodged in your uterus than it is to stop taking a pill. The process of removing an IUD is often no more complicated than pulling on the exposed strings, and some researchers have begun to explore how to make self-removal more feasible. But for now IUD extraction requires an appointment with a health care provider—an appointment that some women struggle to access or afford. Even then, several qualitative studies have found that many women who want to stop using their IUD because of side effects face resistance from their doctor.
In a pair of recent studies, Jennifer R. Amico, an assistant professor at Rutgers Robert Wood Johnson Medical School, and her colleagues interviewed providers and women seeking “early” IUD removal—within nine months of insertion—at two clinics in New York City. Many of the women said their providers minimized their side effects and were reluctant to grant their request for removal. The providers, many of whom admitted they had negative feelings about early removals, said they usually encouraged patients to stick with the device for at least three to six months.

The belief that side effects will improve for most IUD users after an “adjustment period” is widely held by providers. But most studies claiming to show such a decline in side effects over time have not accounted for the dropping out of dissatisfied users. In other words, it could be an illusion produced by the fact that those who do continue to have side effects eventually remove the device, leaving only satisfied users at the end. In a 2009 prospective analysis of copper IUD users that sought to correct this bias in prior studies, researchers found that while some problems improved, others did not; women reported that the number of days they experienced spotting and pain between periods actually became more frequent over time.
“There is a long, terrible history of discounting what women report as contraceptive side effects,” Foster says. In the 1950s, when the first large human trials of the original birth-control pill—which contained astronomical levels of hormones by today’s standards—were conducted on Puerto Rican women, their complaints of severe side effects were brushed off as hypochondria. Today, Foster says, “there is a belief that if a clinician tells a woman about side effects, that she is more likely to experience them.” Indeed, a number of published articles in recent years claim that “nonspecific” side effects to oral contraceptives are the result of the “nocebo” effect—a negative placebo effect—and so providers should offer “optimistic” counseling that downplays their likelihood.
The illusion of choice
The “LARC-first” movement is based on the assumption that effectiveness should be the only factor to consider in a contraceptive method. “Folks will often say, ’I wouldn’t give you a statin that is 91 percent effective versus one that is 99 percent, so why would I give a contraceptive that has that difference in efficacy?’” says Anu Manchikanti Gomez, director of the University of California, Berkeley’s Sexual Health and Reproductive Equity Program. But there are many factors—from side effects to health risks to control over starting and stopping the method—that women weigh when choosing among imperfect options.
Gomez, who co-authored a critique of the LARC zeal in a 2014 article entitled “Women or LARC First?” now says that the reproductive health field has begun to see a “pendulum shift toward a patient-centered approach and recognition that what health care providers and policy makers consider to be the ‘best method’ is often misaligned with what women want.” In 2016 the advocacy groups National Women’s Health Network and SisterSong released a statement of principles for IUDs and implants that rejected “efforts to direct women toward any particular method” while supporting greater access to LARC devices. It also emphasized the right of all women to opt against LARC or discontinue using one without judgment from their provider. More than 250 advocates and organizations, including ACOG, have signed on to it.
The reality is that most women who are shopping for birth control likely won’t choose these devices anyway. In a 2015 study, Foster and her team surveyed about 100 experts who had published research on LARC and asked them to estimate how many women would use it if all the current barriers were eliminated. The median estimate was 25 percent. “The idea that LARCs are going to solve all our problems is problematic on a lot of fronts,” Foster says. “It’s also just not realistic.” The solution to better birth control, she adds, lies in soliciting and respecting women’s preferences when it comes to contraception and then using science to develop methods that meet their needs.
That is certainly not the approach we have taken so far. Although investment in research and development by pharmaceutical companies in the 1990s and 2000s yielded new products, such as the patch, ring and hormonal IUD, it has cooled in the past decade. These days “they think that there are enough products for female contraception,” says Régine Sitruk-Ware, a scientist at the Population Council’s Center for Biomedical Research.
Anyway, recent contraception advances have largely been tweaks to the formulations or modes of delivery of the same basic synthetic hormones that have always been used. And projects in the pipeline are similarly focused on making existing contraceptives easier or safer. For example, a self-administered injectable, recently approved in other countries, could hit the market in the U.S. A “pericoital” pill, similar to emergency contraception, that needs to be taken only when someone has sex is under development. So is a ring that uses natural estradiol—bioidentical to the estrogen in the human body—instead of a synthetic estrogen, which may be a safer option for women put at an increased risk of blood clots by many existing hormonal contraceptives.
Experts say the focus has been on improving existing hormonal methods largely because they are well understood at this point. Efforts to develop brand-new ones will face a long and expensive path to reach the market. But all the scientific progress since the pill was developed could yield much more imaginative strategies.
Toward innovative birth control
Recent advances in genomics have identified many proteins, enzymes and genes involved in the reproductive process that could be targeted to prevent pregnancy in both women and men—and potentially do so in more precise ways. Sitruk-Ware says her group is exploring a molecule that, by acting on a particular protein, would prevent sperm from maturing, making them unable to fertilize an egg. Another research team has been testing a compound in nonhuman primates that binds to different protein and turns off sperm’s ability to swim. “There may be as many as 1,000 possible targets,” Blithe says, including some “very exciting possibilities” when it comes to inhibiting ovulation that are at the basic research stage.
None of these compounds has made it through preclinical toxicology studies to get into a human trial yet. “We are expecting that they would be safer because we are targeting and blocking only one specific protein, and there will be no other action on any other cells in the human body,” Sitruk-Ware says. “But it’s unknown—any molecule may bring other effects.”
Genomic approaches could someday bring a precision medicine approach to prescribing contraception as well. Genetic variations may explain why the side effects of contraceptive methods vary widely among individuals—and genetic testing might help predict which method is best for a particular woman. For example, although such testing is not available in routine practice, doctors already have the ability to test for specific mutations that put women at higher risk of blood clots on estrogen-based contraceptives. And genetic variations may explain why no birth control is 100 percent foolproof. A study published online in March in Obstetrics & Gynecology found that about 5 percent of women possess a genetic mutation that makes them more likely to produce an extra hormone-dismantling enzyme that makes birth control less effective. Previously, women who got pregnant on the pill were blamed for not using it correctly.
Technological advances are also bringing more precision to one of the oldest contraceptive methods: fertility awareness. A couple can only fertilize an egg up to about five days before and two days after ovulation because of the combined viability of sperm and egg in the female body. So the goal of fertility awareness–based methods, or FABMs, is to predict—and then confirm—when ovulation occurs. Many FABMs do so by tracking physical signs of hormonal shifts, including changes in cervical fluid and a spike in basal body temperature. When done right, some are 95 to 99 percent effective.
FABMs are one of the only contraceptive methods besides LARC whose popularity is on the rise. An estimated 3.2 percent of women using contraception use a FABM today, a figure that doubled between 2008 and 2014. The interest is likely being driven in part by the variety of fertility- and period-tracking apps now available. Some just provide a digital platform to chart one’s cycle, whereas others utilize predictive algorithms. “There’s machine learning going on in the app that helps it adapt to the woman’s cycle,” explains Victoria Jennings, director of the Institute for Reproductive Health at Georgetown University Medical Center.
Jennings doubts the new algorithm-based apps are more effective than old-school FABMs that require a woman to chart her cycle with paper and pencil, but “they’re so much easier to use that, in my opinion, people may be more likely to use them correctly.” So far few apps have undergone rigorous efficacy testing. She and her colleagues recently completed a first-of-its-kind prospective study of one such app called Dot. The results, published online in March 2019 in the European Journal of Contraception and Reproductive Healthcare, found a perfect-use failure rate of 1 percent and a typical-use failure rate of 5 percent.
Even with an app, FABMs are as far from “set it and forget it” as you can get. Because a woman’s cycle is affected by factors such as stress, lack of sleep and illness, algorithms cannot confidently predict the exact day of ovulation for each cycle based on historical patterns alone. That is where scientific advances could help. Current at-home urine tests can anticipate ovulation by a couple of days at most. But that won’t cut it if a couple is trying to avoid pregnancy instead of achieve it. “I would love to see some kind of a hormonal test that could accurately predict ovulation far enough in advance for people to be able to rely on it for pregnancy prevention at a cost that they could afford,” Jennings says. That would achieve the same goal as FABMs at a fraction of the effort.
Of course, one way to relieve some of the burden on women to prevent pregnancy is to share it with their male partners. Hormonal birth control for men is much further along in development than nonhormonal approaches for either sex. “We have a lot of small studies that demonstrate it works and in a similar way to female methods,” Blithe says. Late last year the second phase of a clinical trial of 420 couples to test the safety and efficacy of a male contraceptive gel, developed by the Population Council and NICHD, got underway. But the oft-repeated joke in the field is that male contraception has been 10 years away for 30 years. “I’m not promising anything in the next five years for men,” Blithe says.
Among the barriers to developing a male contraceptive has been that the regulatory pathway is uncertain. When the FDA evaluates the safety of a female contraceptive method, any health risks are compared with the risks the woman could experience from pregnancy to calculate the risk-benefit ratio. But in the case of a male contraceptive, “the FDA is going to have a very high bar, I’m sure, when it comes to getting approval for a drug that will be taken by the person who is not at risk of pregnancy,” Blithe says. The pharmaceutical industry has also yet to be convinced there is a big market. A 2005 survey of men in nine countries found that 55 percent would be willing to use a male hormonal contraceptive. (Their current options are only condoms and vasectomy.) More recent market research by the Male Contraceptive Initiative found almost four in 10 men in the U.S. would be interested, but they also reported “little tolerance for side effects,” especially depression, reduced libido or acne.
Researchers acknowledge that a male contraceptive may need to meet a higher standard than its female counterparts. To many women, the benefit of pregnancy prevention is great enough that they’re willing to put up with nausea, mood swings or heavier periods as the trade-off. “But men? Not necessarily,” says Sitruk-Ware, who co-founded the International Consortium of Male Contraception. “If they make this effort of taking the burden of the couple’s contraceptive method, they would expect that there are absolutely no side effects.”
Female contraceptives should have to clear that high bar, too. Birth control, in general, presents a more complicated risk-benefit analysis than other medications. In exchange for treatment for a life-threatening illness, people may accept considerable side effects and health risks. But “contraceptives are not designed to treat a disease, and the users are typically young and healthy,” Sitruk-Ware says. “Zero side effects should be the rule.”
This push for contraceptive innovation is not universally evident. Many investors believe that to reduce unintended pregnancies, we simply need to ensure that women have access to existing methods. But dissatisfaction is also a reason people use contraception inconsistently or forgo it entirely. Safeguarding and expanding access, though vital, need not crowd out the pursuit of better birth control—a truly diverse range of options that meet the differing needs of both women and men at various stages in their reproductive lives. “Adolescents may not want the same method as a woman who is spacing her pregnancies or a woman who has completed her family,” Sitruk-Ware says. Likewise, whereas many women in a committed relationship may consider a male contraceptive a welcome relief, for others, maintaining control themselves over the use of the method is paramount.
It is hoped that researchers—and funders—will develop targeted ways of preventing pregnancy, along with the ability to more precisely match formulations to individuals’ unique physiology. For now a more personalized approach is critical to help women choose among the current lineup of choices, which force too many of us to trade well-being for effectiveness. Finding a contraceptive method that best fits someone’s body, way of life and priorities is a complex task—and shouldn’t be compared to setting a chicken in an oven and walking away.
 Rights & Permissions
Rights & Permissions

